Our Goal
Circulation
Symptoms
Term Vascular Health
Are You Experiencing These Symptoms of Peripheral Artery Disease (PAD)?
Peripheral Artery Disease occurs when blood flow to the legs is reduced due to narrowed or blocked arteries.
This can lead to pain, poor healing, and worsening circulation over time.
Common warning signs include:
- Pain or cramping in the legs when walking
- Leg fatigue or weakness
- Coldness in the lower leg or foot
- Slow-healing wounds or ulcers on the feet
- Numbness or tingling in the legs
- Skin discoloration on the legs or feet
- Reduced hair growth on the legs
- Pain that improves with rest but returns during activity
Risks of Peripheral Artery Disease
Early diagnosis can prevent serious, life-altering complications.
Risk factors include:
- Smoking
- Diabetes
- High blood pressure
- High cholesterol
- Age above 50
- Family history of vascular disease
- Obseity or sedentary lifestyle
Without Treatment,
PAD May Lead To:
- Chronic leg pain
- Poor wound healing
- Tissue damage
- Increased risk of heart attack or stroke
- Severe cases may result in limb loss

- Early treatment can restore circulation and prevent these complications.
- Seeing a vascular specialist early helps ensure accurate diagnosis and
timely treatment.
Book Your PAD Specialist Consultation Today
If you are experiencing leg pain when walking, numbness, or slow-healing wounds, these may be signs of Peripheral Artery Disease (PAD).
Early diagnosis and treatment can restore circulation and prevent serious complications.
- Early diagnosis helps prevent long-term damage
- Timely treatment improves mobility and quality of life
- Consultations may be available within the same week
Book a PAD Consultation Now
Fast diagnosis • Minimally invasive treatments • Personalised care
Meet Our Vascular Specialists
Both doctors have extensive experience managing complex vascular conditions including PAD.

Dr Benjamin Chua
Medical Director & Senior Vascular Surgeon
Founding Head, Department of Vascular Surgery (SGH)
- Over 20 years of clinical experience in vascular surgery
- Pioneer in vascular care in Singapore (SGH founding head)
- Expertise in complex vascular and endovascular procedures
- Lead author in international vascular journals

Dr Chen Min Qi
Senior Vascular & Endovascular Specialist
Former Head of Vascular Service, Woodlands Health
- Specialist in vascular and minimally invasive procedures
- Experienced in treating arterial diseases and PAD
- Expertise in image-guided interventions
- Strong focus on early diagnosis and holistic patient care
How Peripheral Artery Disease (PAD) is Diagnosed
Accurate diagnosis is the first step to effective treatment.
Our specialists use safe, non-invasive tests to assess blood flow and detect blockages early.
Ankle-Brachial Index (ABI) Test
Ultrasound, CT or MRI Scan
Effective Treatment Options for Peripheral Artery Disease
We offer minimally invasive endovascular treatments designed to restore blood flow and relieve symptoms.
These may include:
- Angioplasty to widen narrowed arteries
- Stent placement to keep arteries open
For many patients, this can be done as a day procedure with same-day discharge. Some patients may require an open surgical bypass surgery when angioplasty/stenting is unsuccessful.
Why Choose
Vascular & Interventional Centre (VIC)
Patients choose VIC for:
Experienced, Professional
and Compassionate Team
Our doctors are experienced with in-depth training. They are supported by a dedicated team of staff, providing customized high-quality care for our patients.
Well-Regarded Facilities
Our modern facility houses the up-to-date Philips Fluoroscopy System, enabling high-resolution and reliable for our doctors to perform complex procedures, leading to enhanced outcomes.
Optimal Results
With minimal invasive treatments from our in-house hybrid OT, to recovering in our comfortable day
suites, patients benefit by recovering quickly within the day.
Reshaping Vascular
Treatments
We are continually advancing methods to treat a comprehensive range of vascular conditions.
Patient Centric &
Evidence-Based Treatment
Personalised treatment plans unique to every individual, which empowers informed decision making and optimal outcomes.
Case Studies – Real Patient Outcomes
See how early diagnosis and treatment helped patients restore circulation and avoid serious complications.
Diabetic Patient with Critical Limb Ischemia
A patient with long-standing diabetes presented with severe reduced blood flow and a non-healing wound in the right leg.Severe PAD with Rest Pain and Previous Amputation
Patient presented with bilateral PAD and rest pain and weeping from a previous left big toe amputation. He has a background history of diabetes mellitus, hypertension and hypercholesterolaemia.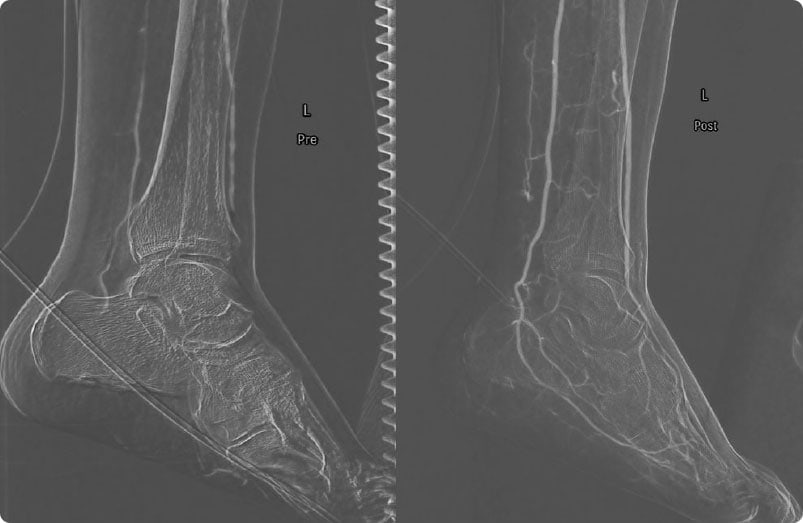
Early Detection of Peripheral Artery Disease
Peripheral arterial disease (PAD) in the legs results from the narrowing and hardening of arteries supplying blood to these areas. When this happens, the legs are unable to receive the necessary nutrients and oxygen that they need, often causing pain. The symptoms of PAD can vary from mild to severe.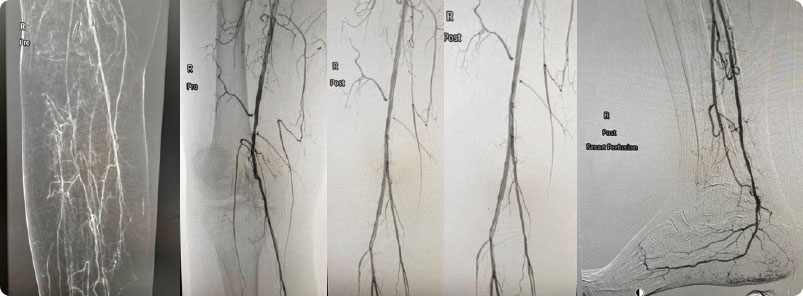
Book Your PAD Specialist Consultation
If you are experiencing leg pain, numbness, or slow-healing wounds, it may be a sign of Peripheral Artery Disease (PAD).
Early diagnosis can prevent serious complications and restore healthy blood flow.
"*" indicates required fields
Appointments may be available within the same week.




