
Uterine fibroids are non-cancerous tumours of the uterus, with a prevalence of 40-50% among women by the age of 35. There are four types of uterine fibroids based on their location: subserosal, intramural, submucosal, and pedunculated.
The following symptoms may indicate the presence of uterine fibroids:
- Abnormal menstrual cycle (heavy or frequent bleeding)
- Painful menstrual periods
- Pain during or after sexual intercourse
- Frequent urination, caused by pressure on the bladder
- Acute or severe pelvic pain
- Bloating
However, in some women, these fibroids may be asymptomatic.
The exact cause of uterine fibroids is unknown, however, these factors may influence your risk of developing fibroids:
- Age
- Heredity
- Obesity
- Vitamin D deficiency
- Excessive alcohol consumption
- Smoking
- No pregnancy history
Ultrasound scan of the uterus
CT scan in the case of multiple fibroids
There are multiple ways to treat uterine fibroids, which usually involve the removal of the fibroids through surgery. Surgical removal of the fibroids is known as myomectomy, while in more severe cases, the entire uterus can be removed in a procedure known as a hysterectomy. Recovery from this procedure usually takes several weeks, and pregnancy is no longer an option.
At VIC, we offer a minimally invasive alternative, Uterine Fibroid Embolisation (UFE). UFE is performed by accessing the groin or radial artery through a puncture. A catheter is then guided using fluoroscopy to the arteries supplying the uterus and fibroids, and microspheres are injected into the fibroid-supplying arteries, cutting off their blood supply and causing shrinkage. This procedure allows a much faster recovery time as compared to traditional surgery – the normal 2-3 week recovery time is shortened to less than a day, with most patients able to leave without overnight stay. Additionally, this procedure poses a lower risk of infection with no scarring, while providing significant symptom relief for 85-90% of women.
Suitability for UFE:
- Women over 35 years old
- Not currently pregnant
- Diagnosed with uterine fibroids and experiencing symptoms
- Prefer non-surgical treatment preserving the uterus
Case Study 1
Patient presented with extremely heavy periods, iron deficiency, and dysmenorrhea. An ultrasound scan was performed, and subserosal and intramural fibroids were discovered. The decision was made to undergo uterine fibroid embolisation.
Embolisation of bilateral uterine arteries and further embolisation of left uterine artery was performed using embolisation particles. Angiogram was performed to ensure the arterial blood supply to the fibroid had been blocked off.
Shrinkage of fibroids was observed when the patient returned for check up after 4 weeks. On MRI adter 3 months, the heavy periods had reduced and iron-deficiency anaemia improved. All without having the need for open surgery.
Case Study 2
Patient presented with multiple fibroids and extensive adenomyosis. Uterine fibroid embolisation was chosen as the method of treatment.
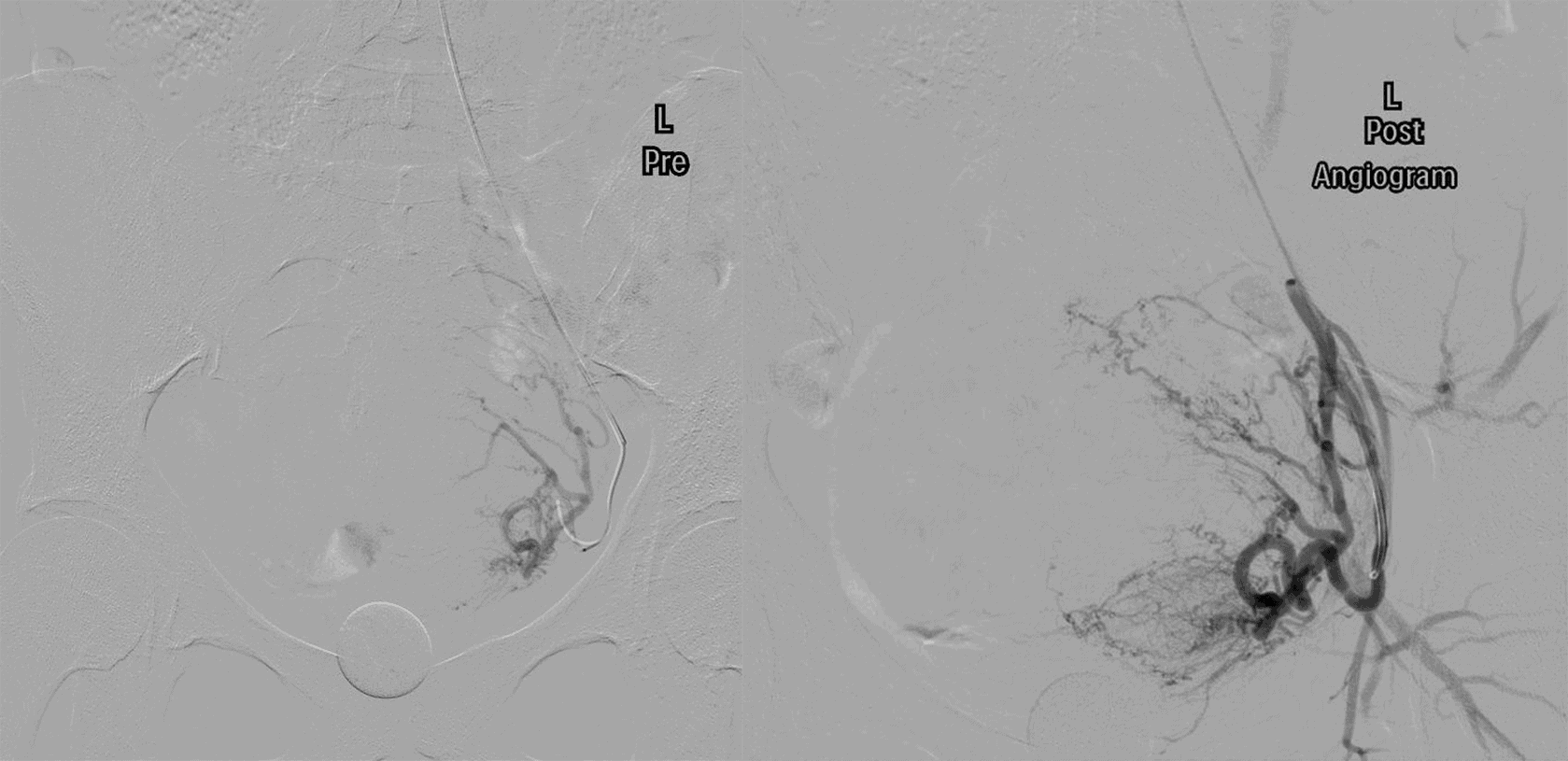
The left uterine arteries supplying the left sided fibroids were cannulated and the fibroids were embolized with micron particles. The left ovarian branch was preserved. The decision was made not to further embolize fibroids to avoid risking the left ovarian artery supply.
Three large fibroids were able to be embolised while preserving ovarian arterial flow. MRI at 3 months showed reduction in size of fibroids.




